Treatment Resistant Schizophrenia (TRS) and Clozaril (Clozapine)®
Defining TRS
The National Institute for Health and Care Excellence (NICE) defines ‘treatment resistance’ in schizophrenia patients as the lack of satisfactory clinical improvement following sequential treatment with at least two different antipsychotic drugs, including at least one second-generation (atypical) antipsychotic.1
TRS is common among schizophrenia patients
Treatment resistance is a significant barrier to effective treatment. A review of several cohort studies estimates that 20-30% of patients with schizophrenia meet the criteria for treatment resistant schizophrenia (TRS).2
Given that an estimated 25‒50% of schizophrenia patients attempt suicide and 10% eventually achieve this goal,3 it is essential that patients with TRS are identified in a timely manner so that they can receive appropriate therapy.
NICE recommends clozapine as first-line treatment for TRS
NICE guidelines recommend that clozapine should be offered first-line to schizophrenia patients who have not shown satisfactory clinical improvement following sequential treatment with at least two different antipsychotic drugs, including at least one second-generation (atypical) antipsychotic.1
Clozapine is underutilised in the United Kingdom
In 2018/19, only 54% of eligible patients in England were prescribed clozapine, which has improved slightly to 60% in 2023/24,4 so there is still room for improvement.
Under-prescription of clozapine may be due to a combination of patient-, clinician-, and health system-related factors.5
The rate of clozapine prescribing is lower in England than other parts of the UK. For example, there has been a marked improvement in clozapine prescribing in Wales, from 55% in 2018/19 to 87% in 2023/24.4
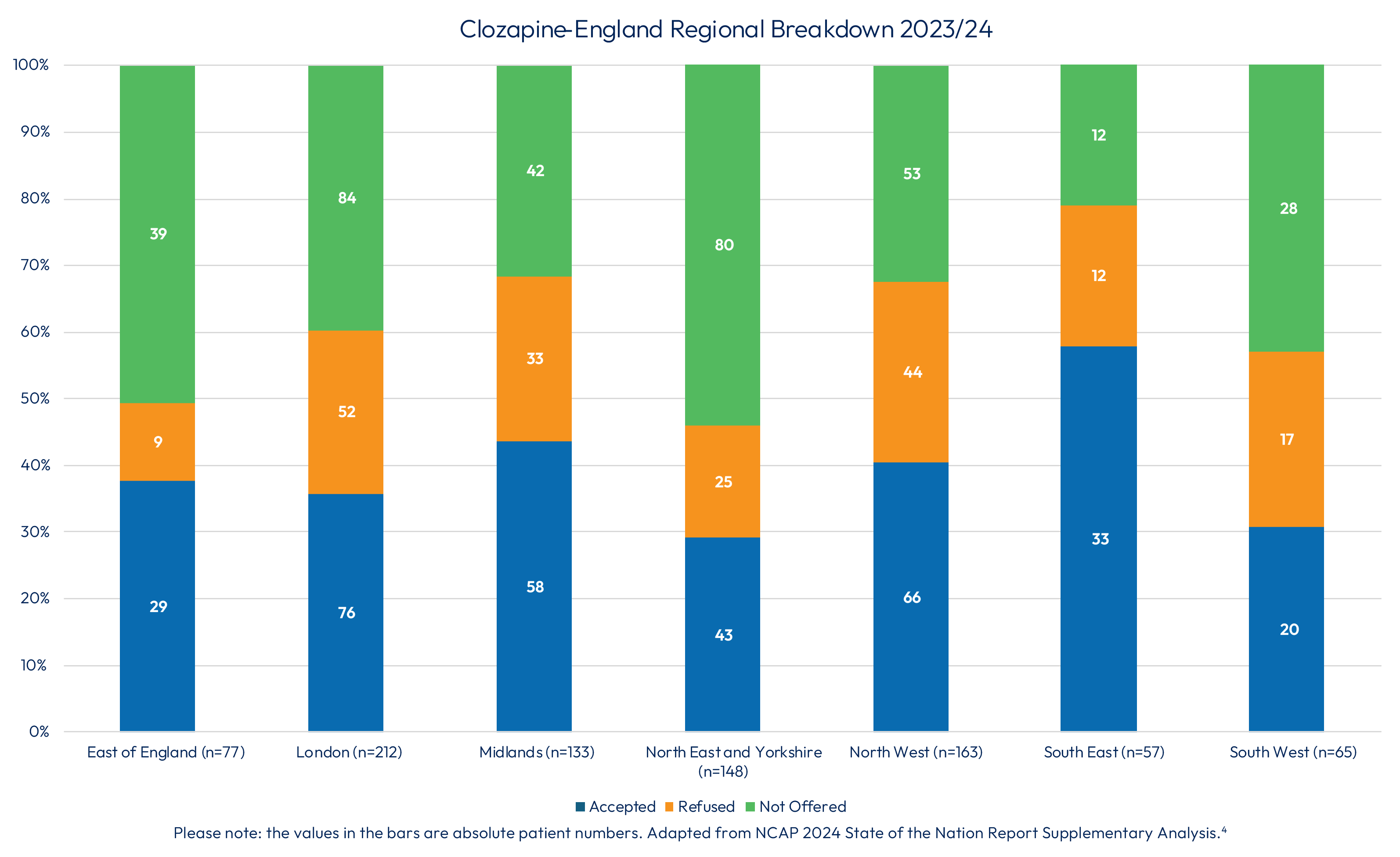
Offering clozapine to eligible patients varies across England:4
Blood monitoring while on Clozaril® is mandatory
White blood cell abnormalities are possible with clozapine treatment so all patients receiving it must be monitored regularly for white blood cell (WBC) count and absolute neutrophil count (ANC).6
Pre-treatment blood testing
WBC and differential blood counts must be performed within 10 days prior to initiating Clozaril® treatment to ensure that only patients with normal WBC count (≥3500/mm3 [3.5x109/l]) and ANC (≥2000/mm3 [2.0x109/l]) receive Clozaril®.6
Blood monitoring after Clozaril® initiation
After the start of Clozaril® treatment, regular WBC count and ANC must be performed and monitored weekly for the first 18 weeks, and at least four-weekly thereafter.
Monitoring must continue throughout treatment and for 4 weeks after complete discontinuation of Clozaril® or until haematological recovery has occurred. WBC and differential blood counts must be performed immediately if any symptoms or signs of an infection occur.6
Action if a patient has low WBC count/ANC
If a patient develops a low WBC count and/or low ANC while on Clozaril® treatment, monitoring must be increased to at least twice weekly until counts recover to within an accepted range. If WBC count and ANC fall below a specific threshold, Clozaril® must be discontinued immediately.6
Table 1 summarises the actions required for WBC counts and ANC thresholds.
Table 1. Blood cell parameters and actions required for patients receiving Clozaril®6
Blood cell count
WBC/mm3 (/l)
ANC/mm3 (/l)
Action required
≥3500 (≥3.5x109)
≥2000 (≥2.0x109)
Continue Clozaril® treatment
Between ≥3000 and <3500 (≥3.0x109 and <3.5x109)
Between ≥1500 and <2000 (≥1.5x109 and <2.0x109)
Continue Clozaril® treatment, sample blood twice weekly until counts stabilise or increase.
<3000 (<3.0x109)
<1500 (<1.5x109)
Immediately stop Clozaril®
treatment, sample blood daily until
haematological abnormality is
resolved, monitor for infection. Do not
re-expose the patient.
If Clozaril® has been withdrawn and either a further drop in the WBC count below 2000/mm3 (2.0x109/l) occurs or the ANC falls below 1000/mm3 (1.0x109/l), the management of this condition must be guided by an experienced haematologist.
Farooq S, Choudry A, Cohen D, et al. Barriers to using clozapine in treatment-resistant schizophrenia: systematic review. BJPsych Bull 2019;43(1):8-16.